


Theme
Medical Physics
INSTITUTION
Royal Hospital/ Muscat

The radiation oncology department at the Royal Hospital in Muscat, Oman, obtained a Varian TrueBeam ver. 2.5 SRT linac in 2016. Two megavoltage x-ray beams, 6 MV and 6 FFF, were commissioned on an Eclipse treatment planning system (Ver 13.7) using dosimetric data ranging from 40x40 cm2 to 4x4 cm2 as recommended by the vendor.
Although a dedicated iPlan treatment planning system is routinely used for stereotactic radio-surgery (SRS) planning, we wanted to investigate the feasibility of using our Eclipse treatment planning system for the treatment with small fields. These fields are typically used in SRS treatments and have dimensions smaller than those recommended by the vendor.
Percentage depth doses PDDs, off-axis ratios OARs and output factors were measured for the 6 MV and 6 FFF megavoltage x-ray beams using a pinpoint chamber for 3x3 cm2, 2x2 cm2 and 1x1 cm2 fields. Separate beams were configured in the Eclipse planning system with one being configured with beam data containing the vendor recommended dosimetric data ( fields between 40x40 and 4x4 cm2) and the other with dosimetric data for the small fields in addition to vendors recommended dosimetric data.
To test the performance of the Eclipse treatment planning system we first compared the PDDs for 3x3 cm2, 2x2 cm2 and 1x1 cm2 fields with the measured data used in configuring the Eclipse beam models. In addition, VMAT plans for single and multiple SRS type lesions were optimized and calculated with the Eclipse planning system. The optimized plans were then recalculated in a standard 30x30x15 cm3 QA Solid Water phantom. Using a small thimble ionization chamber, measured and calculated doses within the QA phantom were compared to one another.
Measured PDDs for 6 MV and 6 FFF beams were compared to Eclipse calculated PDDs for beam configured with small fields dosimetric data. The calculated PDDs for depths 5 and 10 cm and 3x3 cm2 field size were less than 0.2% from measurements, however, for the 2x2 cm2 field size the discrepancy increased to 1.0%. TABLE 1 lists calculated and measured PDDs at depth of 10 cm for 6 MV x-ray beam.
| PDD | ||
| Field size (cm2) | Measured | Calculated |
| 2x2 | 60.2 % | 59.5 % |
| 3x3 | 60.4 % | 60.3 % |
Moreover, plans optimized and calculated with 6 MV beam configured with small field dosimetric data, the calculated and measured doses in the QA phantom were in closer agreement with one another in comparison to plans optimized with 6 MV beam configured without including small fields dosimetric data.
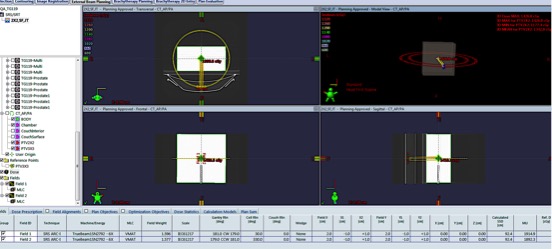
Fig. 1: VMAT plan with two 2x2 cm2 field size arcs without jaws-tracking.
We also noticed that the agreement between calculated and measured doses improved when jaw-tracking is disabled in plan optimization for field sizes 3x3 cm2 with discrepency between 1% to 3%. For fields smaller than 3x3 the difference between calculation and mesaurements are of the order of 5% regardless the jaws tracking option used in optimization.
| Field size 2x2 cm2 | commissioned with small field data | commissioined with vendor recommended data only |
|---|---|---|
| With jaws-tracking | 6.2% | 6.0% |
| without jaws-tracking | 6.0% | 5.3% |
It is important to include dosimetric data for small fields in treatment planning beam data when planning to treat small lesions. To further reduce discrepancies between calculation and measurements, we recommend using fixed-jaws positions when optimizing plans for small lesions.
- A fine calculation grid size is recommended to be used.
- Fixed collimator jaws at 3 × 3 cm2 should be used for small target volumes where the jaw tracking leads to jaw defined field sizes smaller than 3 × 3 cm2.
(1) Hao Wu et al, A comparative study of identical VMAT plans with and without jaw tracking technique, Journal of applied clinical medical physics, Voulme 17(5), 2016.
(2) Ans C.C et al, Influence of the jaw tracking technique on the dose calculation accuracy of small field VMAT plans, Journal of applied clinical medical physics, Voulme 18 (1), 2017.
 Send Email
Send Email