
| Theme: 4BB Teaching tools | |||
 |
||||||
| Video conferencing applications to establish a distributed educational network: enhancing early referral of those with acute diabetic foot |
 |
|||||
|
||||||

Background
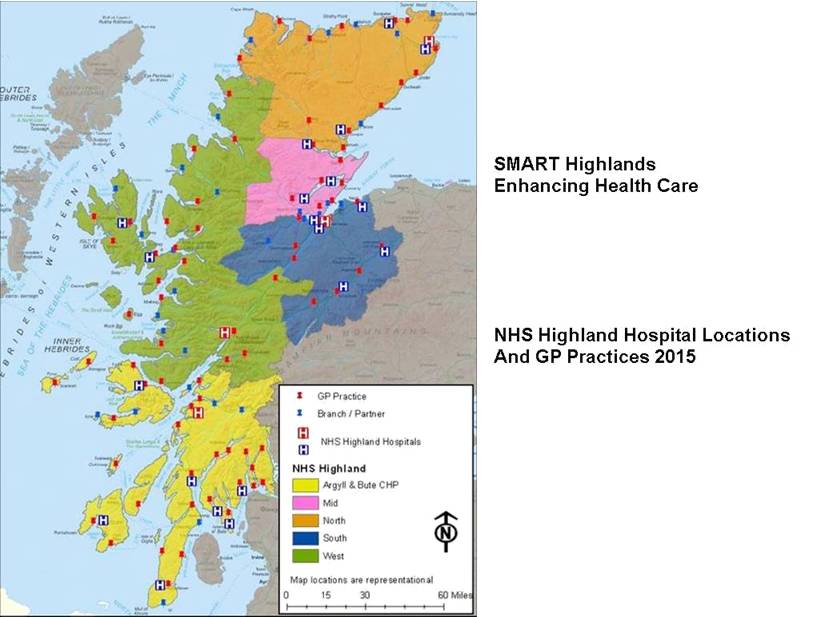
Diabetes Foot Education Network
(DFEN)
- NHS Highland evidence based clinical guidelines management of the foot in diabetes (developed 2013)
- Need to increase Healthcare Professional (HCP) familiarly and application of guidelines
- The Scottish Diabetes Improvement Plan 2014 pledges to ensure delivery of consistent, high quality diabetes education
- Early referral to reduce amputation rates
Purpose of DFEN
- Increase awareness and application of existing local & national guidelines
- Provide facilitated specialist education
- Provide opportunity for at distance staff networking and sharing best practice
- Promote and increase rates of early referral
Summary of Work
Delivery Plan
- Lead diabetes clinicians collaborated with Remote & Rural Health (RRHEAL) and NHS Education Scotland (NES) to increase educational reach and resulting clinical application
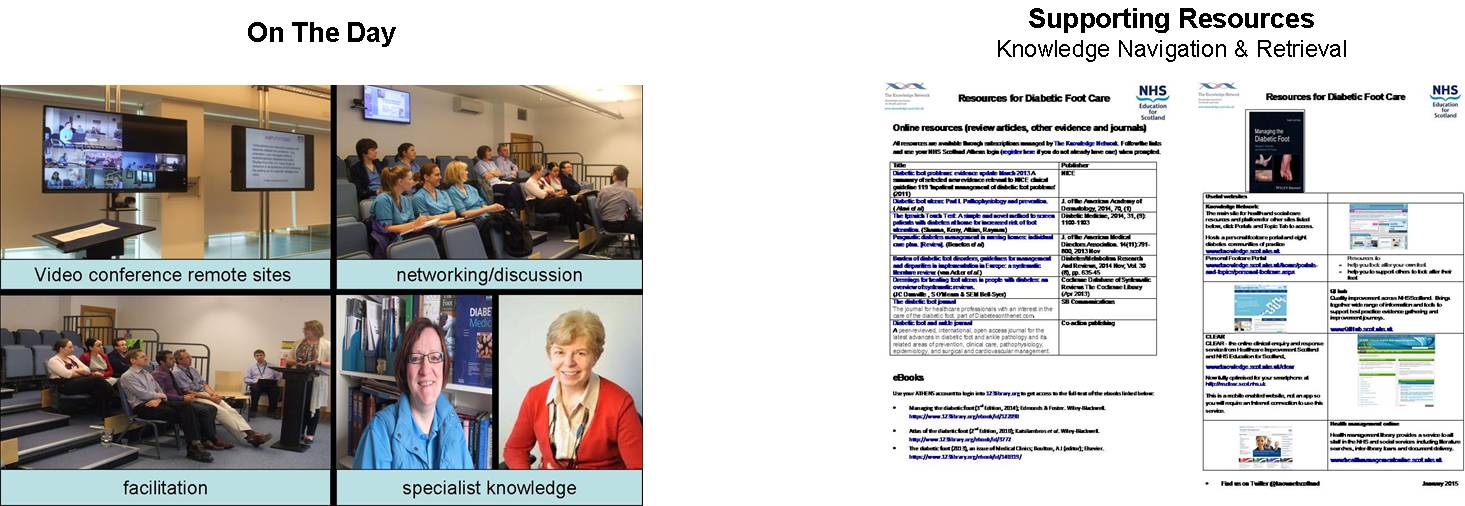
- Video Conferencing (VC) was an accessible medium to enhance networked mixed discipline engagement
- Expert knowledge existed within the team to deliver open, case based approaches across an annual programme supporting critical discussion
- Presentations are person focused, guideline specific, educational and instructive in terms of guideline application
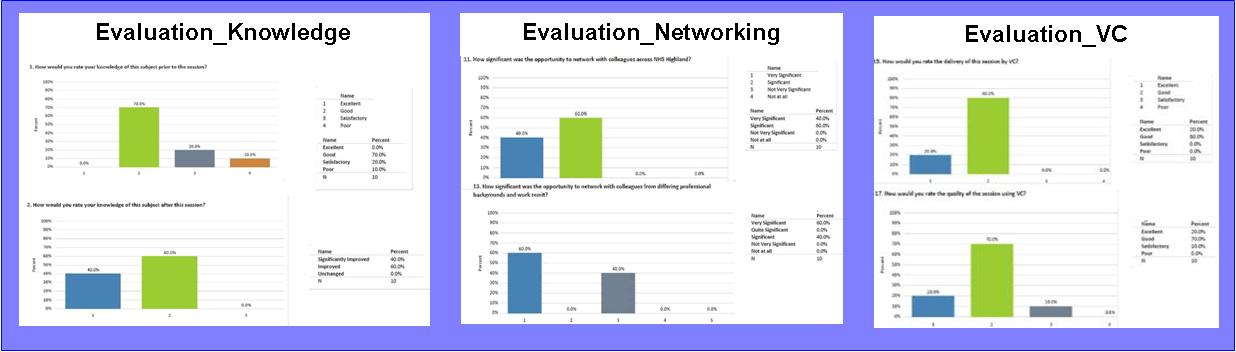
Summary of Results
Take-home Messages
- This work delivers an educational intervention that is cost neutral, accessible and inclusive for staff by geography and profession
- Enhances knowledge and application of guidance for early referral
- Offers the opportunity to network and engage at distance
- Connection between remote practitioners and the Specialist hub, enhancing communication and clinical practice or application
- Knowledge support enhances retrieval & application of evidence based guidelines to the benefit of staff teams and, ultimately, the diabetes population
References
- Diabetes Improvement Plan 2014, Scottish Diabetes Group
- NHS Highland Shared Clinical Guidelines (2014) http://intranet.nhsh.scot.nhs.uk/Clinical/SharedClinicalGuidelines/Diabetes/Pages/Default.aspx accessed 28/08/2015
- Developing Professionals for diabetes care in NHS Highland (a learning needs assessment)
- Educational Governance (2014) Educational Governance Framework NHS Highland.
- NHS Education for Scotland Inclusive Education Policy (2012) http://www.nes.scot.nhs.uk/about-us/equality-and-diversity/inclusive-education-and-learning.aspx accessed 28/08/2015
 Send Email
Send EmailDesigned & Managed by Innovative Technology®